What comes to your mind when you read or hear “Pelvic Tilt”?
Do you think about a leg length discrepancy? Or Trendelenburg gait? or the ranges through which a pelvis can “tilt”?
A pelvic tilt can indicate bone alignment and muscle function status during an MSK assessment. In addition, the context in which it is being assessed can also provide information about a person.
A pelvic tilt variation is physiological in some instances, like exercise, sports, yoga, etc. Although, in some other cases, a pelvic tilt variation can indicate a musculoskeletal pathology.
This article will cover the topic of pelvic tilt across posture, gait and running.
What is a pelvic tilt?
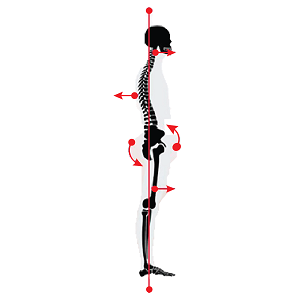
It is the orientation of the pelvis with respect to the femur and the rest of the body. It is the angle between a line from the sacral endplate midpoint to the centre of the bifemoral heads and the vertical axis.
In an anatomical position, the resting position of the pelvis is aligned anteriorly by 7 to 19 degrees [1] in the sagittal plane and neutral in the frontal plane.
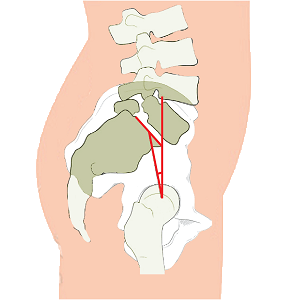
Pelvic tilt is the angle created by a line from the sacral endplate midpoint to the centre of the bifemoral heads and the vertical axis
Types of pelvic tilt

ANTERIOR PELVIC TILT
Observed in saggital plane. It is when the pelvis tilts more anteriorly from its resting position.
POSTERIOR PELVIC TILT
Observed in saggital plane. It is when the pelvis tilts posteriorly from its resting position.

LATERAL PELVIC TILT
Observed in the frontal plane. It is when the pelvis tilts either to the left or the right side from its neutral position. The side of the tilt is determined by the side which is lower. For e.g., if the left side is lower, it is a “Left lateral pelvic tilt”.
Variations in pelvic motion
It’s easy to believe that everyone should have an “Ideal Posture”, which entails perfect alignment. Although theoretically and practically, it’s impossible to expect the whole 8 billion population to have the exact alignment. Therefore, knowing how much a range can vary is essential before deeming the posture as pathological.
The average range of maximum anterior and posterior pelvic tilt achieved through active motion are 21.2 ± 6.4°, and -0.7 ± 6.5° respectively. [2]
Pelvic Tilt in Posture
This is a hot topic for debate. However, pelvic tilt is a standard assessment in patients with low back pain, and any deviation beyond “ideal” alignment is considered pathological.
Physiological Pelvic Tilt in Posture
In a standing posture, the pelvis is anteriorly tilted between 7 to 19 degrees, on average, in the sagittal plane and neutral in the frontal plane. As stated in the previous section, variations beyond these are also considered normal.
Common presentations with Anterior Pelvic Tilt
- Increased lumbar lordotic curve
- Tibial Abduction
- Foot pronation
Common presentations with Posterior Pelvic Tilt
- Decreased lordotic curve
- Tibial Adduction
- Foot Supination
Pathological Pelvic Tilt in posture
A position of the pelvis beyond the ranges, including variations, can be an effect of musculoskeletal or neurologic conditions.
1. Deviations in the sagittal plane [3]
Lordotic Posture
Lordotic Posture
Marked by a significant increase in anterior tilt of the pelvis. This posture can increase compressive loads on lumbar discs and increase shear stress in the L5-SI Junction.
Flat Back Posture
FLAT back Posture
Marked by a neutral or slightly posteriorly tilted pelvis. This posture reduces movement variability in the spine.
Swayback posture
Sway back Posture
Marked by a posterior pelvic tilt and increased thoracic kyphosis. Interestingly, this may be caused by an anterior shift of the pelvis, a longer thoracic kyphosis extending up to the upper lumbar spine, or a shortened lumbar spine.
This posture reduces movement variability of the pelvis and can increase compression on the posterior elements of the vertebrae.
Ankylosing spondylitis posture
Ankylosing spondylitis
A genetic condition in which the spinal curves are flattened, giving it an appearance of a rod. The pelvis tilts posteriorly.
2. Deviations in the frontal plane
These deviations often stem from structural problems and are less common from muscular problems. When the pelvis is not in neutral in the frontal plane, it is termed ‘Pelvic Obliquity’.
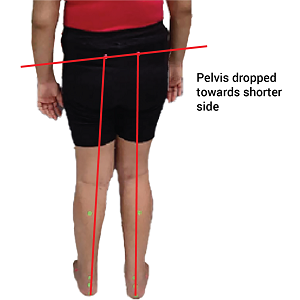
LEG LENGTH DISCREPANCY
The pelvis is dropped on the side of the shorter limb
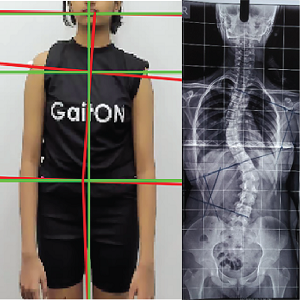
SCOLIOSIS
The pelvis drops on the side of the convexity of the scoliotic curve.
Compensatory Pelvic Tilt
These are cases in which a change in pelvic tilt occurs for biomechanical reasons, and may not need correction most of the time, as they’re helping relieve the pathology than aggravating it.
For example, in Patello-femoral joint OA, an anterior pelvic tilt reduces the net patellofemoral joint reaction forces and vasti forces, reducing joint loading.
Similarly, children with neurological conditions tend to adopt an anterior pelvic tilt posture to maintain balance and stability.
Muscular contractures or paralysis
The pelvis is dropped on the side of the shorter limb
Pelvic Tilt in Gait
Physiological Pelvic Tilt in Gait [4]
1. In the Saggital Plane
At initial contact, the pelvis is in a position of anterior pelvis tilt. It starts to tilt posteriorly up to 20% of the gait cycle. Then it tilts anteriorly till the contralateral foot contacts the ground, i.e., at about 50% of the gait cycle. The cycle then repeats itself, tilting posteriorly, and anteriorly again.
Between this anterior-posterior movement, the pelvis moves between 2-5 degrees.
2. In the Frontal Plane
The pelvis is neutral (level) during the initial double weight-bearing stage (0 degrees).
After the initial contact, the pelvis drops on the contralateral side by 20% and becomes neutral after the contralateral foot touches the ground. Therefore, it faces a slight drop throughout the swing phase.
The purpose of this drop is to maintain the Centre of Mass and prevent too much up-down displacement. This mechanism forms one of the 6 “Determinants of Gait”, brought about by the motions of the pelvis, knee and ankle, whose purpose is to ensure a smooth gait without excess variations in the Centre of Mass.
Depending on the walking speed, the pelvic drop and return to neutral movement is between 6-11 degrees.
Pathological pelvic tilt in gait
- An excessive lateral drop on the contralateral side (beyond 11 degrees) indicates a hip abductor weakness on the ipsilateral side. This is known as Trendelenburg Gait.
- In response to weak hip musculature, an increase in hip abduction moment and ipsilateral trunk sway is seen during the mid and terminal stance of gait to reduce the contralateral drop.
- In congenital bone deformities, such as acetabular dysplasia, there’s a significant pelvic drop on the affected side
- Neurological conditions present with an increased anterior pelvic tilt.
Pelvic tilt in running
The motion of the pelvis during running is similar to that of the gait, except that the forces are much higher, requiring more muscle activity to stabilize the pelvis.
Physiological pelvic tilt in running
Anterior pelvic tilt peaks during or immediately after the stance phase, i.e., during the early flight phase, and is accompanied by lumbar flexion and hip extension. This causes an increase in femoral inclination during toe-off, thereby increasing stride length.
Posterior pelvic tilt peaks during early stance and is accompanied by thoracic flexion.
Lateral pelvic tilt is observed during initial contact till mid-stance with a slight drop in the pelvis from on the contralateral limb, followed by a sharp rise in the level during toe-off.
Pathological pelvic tilt in running
1. MEDAL COLLAPSE
This is a biomechanical error seen in runners where there is a pelvic drop during the stance phase. While the abductors might be strong enough to keep the pelvis level during walking, they might not be enough to keep the pelvis level during a high-impact activity such as running.
This makes the running less efficient and might lead to an overuse-related strain.
Increased contralateral pelvic tilt and trunk sway compensation
Assessing pelvic tilt [6]
- Visual Assessment – The therapist observes the anterior and lateral views. This is the least reliable method.
- Hand-held Inclinometer – The clinician aligns the inclinometer to the sagittal plane and places it on the sacrum. The numbers indicate the angle of the anterior pelvic tilt. Fairly reliable, but only a few studies have investigated this method’s validity.
- Caliper-based Inclinometer – The therapist aligns the adjustable arms of this type of inclinometer with the ASIS and PSIS and calculates the angle. This method shows excellent reliability.
- 2-D and 3-D Video Analysis – These systems assess pelvic tilt based on markers placed on the ASIS and PSIS. The difference in level between these markers indicates the degree of pelvic tilt.
To conclude, the pelvis is quite essential for stability and mobility with respect to proximal and distal body segments.
We’re happy to inform you that GaitON software also has an inbuilt Gait Analysis module which is now used by 300+ clinicians globally to assess pelvic tilt in patients. It provides patient-friendly reports with reference values, automatic notes, pre-post analysis, excel export options and many more!
Reach out to us today to learn more about the GaitON software and set up your own Posture & Gait Lab!
ABOUT THE AUTHOR
GAYATRI SURESH (PT)
Gayatri Suresh (PT) is a Biomechanist who has completed her B.P.Th from DES College of Physiotherapy and M.P.T (Biomechanics) from SRM College of Physiotherapy, SRMIST. Her field of clinical expertise is in movement assessments through video analysis. Apart from her work at Auptimo, she works as a Clinical Specialist at Rehabilitation Research and Device Development, IIT Madras. She has been conferred with gold medals for her Research presentations and for securing First rank with distinction in her MPT degree respectively
Since you’re here…
…we have a small favor to ask. More people are reading our blogs everyday, and each week we bring you compelling content to help you treat your patients better. Please take a moment to share the articles on social media, engage the authors with questions and comments below, and link to articles when appropriate if you have a blog or participate on forums of related topics. — Team Auptimo
REFERENCES:
1. Vialle, Raphaël MD1; Levassor, Nicolas MD1; Rillardon, Ludovic MD1; Templier, Alexandre MD2; Skalli, Wafa MD2; Guigui, Pierre MD1. Radiographic Analysis of the Sagittal Alignment and Balance of the Spine in Asymptomatic Subjects. The Journal of Bone & Joint Surgery 87(2):p 260-267, February 2005. | DOI: 10.2106/JBJS.D.02043
2. Takaki S Ms Pt, Kaneoka K PhD Md, Okubo Y PhD Pt, Otsuka S Ms, Tatsumura M PhD Md, Shiina I PhD Md, Miyakawa S PhD Md. Analysis of muscle activity during active pelvic tilting in the sagittal plane . Phys Ther Res. 2016 Nov 29;19(1):50-57.
3. Czaprowski D, Stoliński Ł, Tyrakowski M, Kozinoga M, Kotwicki T. Non-structural misalignments of body posture in the sagittal plane. Scoliosis Spinal Disord. 2018 Mar 5;13:6.
4. Lewis, C.L., Laudicina, N.M., Khuu, A. and Loverro, K.L. (2017), The Human Pelvis: Variation in Structure and Function During Gait. Anat. Rec., 300: 633-642
5. Stephen J. Preece, Duncan Mason, Christopher Bramah, The coordinated movement of the spine and pelvis during running, Human Movement Science, Volume 45, 2016, Pages 110-118
6. Suits WH. Clinical Measures of Pelvic Tilt in Physical Therapy. Int J Sports Phys Ther. 2021 Oct 1;16(5):1366-1375.
7. Crossley KM, Schache AG, Ozturk H, Lentzos J, Munanto M, Pandy MG. Pelvic and Hip Kinematics During Walking in People With Patellofemoral Joint Osteoarthritis Compared to Healthy Age-Matched Controls. Arthritis Care Res (Hoboken). 2018 Feb;70(2):309-314. doi: 10.1002/acr.23261. Epub 2017 Dec 29. PMID: 28437567.