Many runners say, “Oh, I just experience ‘normal’ pain after running. Nothing to worry about!” — but this mindset overlooks the importance of running injury prevention. The New York Marathon 2025 saw 59,226 runners cross the finish line — the largest in the world — highlighting how rapidly the sport is growing and why running injury prevention has become more important than ever.
Events like these reiterate that running is one of the most popular sports globally, with participation increasing each year. However, with this surge comes a parallel rise in injuries, making running injury prevention strategies essential for both beginners and experienced runners.
Most runners sustain one or more running-related injuries during their running journey. The first one or two injuries are usually taken seriously, prompting diagnosis, rehabilitation, recovery, and a structured return to running. Yet without proper running injury prevention, re-injuries become common.
As re-injuries occur, pain often becomes normalized — seen as just another part of training — until it escalates enough to disrupt performance. This is exactly where effective running injury prevention can change outcomes and prolong a runner’s career.
So a critical question arises: why are injuries so common in running despite advances in sports science and awareness of running injury prevention?
Which leads to the next question — what evidence-based approaches to running injury prevention can actually reduce risk and keep runners training consistently?
Let’s explore what research has revealed about running injuries and running injury prevention over the past few years.
1. Understanding incidence and prevalence of Running Injuries - 3 decades of research
a. R N van Gent et. al (2007)
19.4 to 92.4% of incidence of running related injuries (RRI)
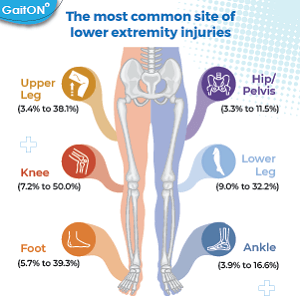
The most common site of lower extremity injuries –
- Knee (7.2% to 50.0%)
- Lower leg (9.0% to 32.2%)
- The foot (5.7% to 39.3%),
- Upper leg (3.4% to 38.1%).
- Ankle (3.9% to 16.6%)
- Hip/pelvis (3.3% to 11.5%)
b. I Buist et. al (2010) -
“At least one RRI was reported by 25.9% of the 629 novice runners during the 8-week observation period. The incidence of RRI was 30.1% per 1000 h of running exposure.”
c. Linda Linton and Stephanie Valentin (2018)
570 out of 1145 runners reported a current injury.
d. Nicholas Kakouris et. al (2021)
Incidence of RRIs – 40.2% ± 18.8%
Prevalence of RRIs – 44.6% ± 18.4%
Highest percent of injury incidence – Knee, lower leg, ankle. Achilles tendinopathy (10.3%), medial tibial stress syndrome (9.4%), patellofemoral pain syndrome (6.3%), plantar fasciitis (6.1%), and ankle sprains (5.8%)
Highest percent of injury prevalence – Knee, lower leg, and foot/toes – Patellofemoral pain syndrome (16.7%), medial tibial stress syndrome (9.1%), plantar fasciitis (7.9%), iliotibial band syndrome (7.9%), and Achilles tendinopathy (6.6%)
e. Mansueto Gomes Neto et. al. - (2023)
“The overall incidence of running-related musculoskeletal injuries ranged from 0.9% to 99%, and the prevalence ranged from 36% to 63.5%. Injuries were most commonly reported at or below the knee. The most common anatomical sites were the knee, followed by the ankle-foot, calf, and upper leg (hamstring, thigh, and quadriceps). The most common types of injuries were plantar fasciitis, medial stress syndrome, patellofemoral pain syndrome, Achilles tendinopathy, sprains, contractures, and ligament injuries.”
2. Causative factors of running injuries
Demographic / Non-modifiable Factors
- Male gender
Running Experience / Exposure History
- No previous running experience
- Low running experience
Training Load & Programming Errors
- Running without adequate rest and recovery periods
- Overtraining
- Rapid increase in mileage/intensity
- High weekly running volume
- Sudden surface changes / excessive downhill running
- Inadequate preseason conditioning
Previous Injury Status
- History of previous injury – unhealed
Biomechanical & Musculoskeletal Factors
- Leg length discrepancy
- Weak hip abductors or calf muscles
- Limited ankle dorsiflexion
Footwear & Equipment Factors
- Inappropriate or worn-out footwear
- Abrupt switch to minimalist shoes
Physiological / Health Factors
- High BMI
- Low bone mineral density / RED-S
Recovery, Lifestyle & Psychosocial Factors
- Alcohol Consumption
- Poor sleep
- Ignoring early pain symptoms
- High life stress / poor recovery
3. Running injury prevention strategies
a. Heather K. Vincent et. al (2022)
- Education on pain monitoring and safe training
- Running mechanics analysis and gait retraining
- Dynamic warm-up (multijoint mobility drills)
- Kinetic chain strengthening (foot → trunk)
- Foot strengthening (intrinsic muscle training, short foot, barefoot drills)
- Core/trunk stabilization
- Neuromuscular strength and balance training (e.g., wobble board, single-leg work)
- Eccentric strength training (especially hamstrings, quadriceps, calf)
- Plyometric training
- Preseason/precompetition neuromuscular preparation
- Cadence control (maintain preferred step rate, especially downhill)
- Step rate increase + forefoot strike to reduce impact
- Terrain-specific practice
- Planned rest intervals to avoid fatigue-related breakdown
b. Linda Linton et. al (2025)
- Education (injury prevention advice/programmes)
- Training strategies (load management, structured training, gradual progression, return-to-run)
- Strength & conditioning (strength, resistance, neuromuscular training)
- Gait retraining (technique modification)
- Footwear & orthotics
- Stretching & warm-up
- Recovery strategies
- Screening & monitoring (risk factor assessment)
- Psychological/behavioural approaches
c. Johnston MD (2003)
1. Gradual training modification is important for running injury prevention
- Graduated training program
- Increase distance/intensity ≤10% per week
- Adequate rest (24–48 hours)
- Avoid “too much, too soon”
- Gradual introduction of new surfaces
2. Correct Biomechanics & Alignment supports running injury prevention
- Assess arch type and leg length
- Use orthoses if indicated
- Use heel lifts for leg-length discrepancy
3. Footwear can affect running injury prevention strategies
- Select shoes based on foot type
- Replace shoes every 500–700 km or 1 year (whichever comes first)
4. Strength & Flexibility is essential
- Lower extremity strengthening (eccentric focus)
- Post-exercise stretching (30–60 seconds per stretch)
5. Training Surface matters
- Choose appropriate surfaces
- Avoid sudden changes in terrain
- Limit hard surfaces when possible
6. Education goes a long way
- Teach runners to recognize early symptoms of injury
Why aren’t running injury rates reducing in spite of all the running injury prevention research?
Inconsistent application in practical settings
Designing running injury prevention programs requires understanding of research, knowing how to interpret, and finally how to apply it in practical settings. Constant updation of knowledge and practice by healthcare providers and coaches is essential.
Normalization of pain
A major barrier to running injury prevention is the normalization of pain within running culture. “It’s just tight.” “It’ll warm up.” “It always hurts at the start.” This mindset delays intervention until tissue breakdown is significant. Research supports education and early pain monitoring — but culturally, endurance athletes are rewarded for pushing through discomfort, not backing off at the first warning sign.
Mismatch between controlled research environments and real-life complexity.
Another challenge in translating running injury prevention research into lower injury rates is that prevention studies often isolate one variable i.e., cadence, footwear, strength training, orthotics yet injuries are multifactorial. A runner might improve cadence but still be sleep deprived. They may strengthen calves but continue rapid mileage increases. They may buy the “right” shoes but ignore recovery. Small risk factors compound over time. Prevention is rarely about one magic fix; it is about cumulative load management across biomechanics, physiology, psychology, and lifestyle.
Finally, long-term running injury prevention programs require consistency, which is difficult. Strength work, neuromuscular drills, and recovery sessions are often the first components dropped when life becomes busy. Mileage, however, is rarely sacrificed. The result? The protective buffer shrinks while mechanical stress remains.
Practical Implications for running injury prevention
1. Reframe Pain Early
Teach runners the difference between adaptive soreness and load-related warning pain.
Normalize modifying training at the first sign of persistent pain — not after performance declines.
2. Load Management is the key to running injury prevention
Weekly load spikes are more predictive than absolute mileage.
Monitor:
- Sudden increases in distance or intensity
- Downhill exposure
- Surface transitions
- Encourage ≤10% progression and planned deload weeks.
3. Strength Is Non-Negotiable when it comes to running injury prevention
Minimum effective dose: 2–3 sessions/week.
Focus on:
- Calf complex (especially eccentric strength)
- Hip abductors
- Quadriceps
- Intrinsic foot muscles
Maintain in-season, not just during rehab.
4. Address Recovery as a Performance Variable
- Sleep quantity and quality
- Energy availability (screen for RED-S)
- Life stress
- Planned rest days
5. Screen for History of Injury
- Previous injury remains one of the strongest predictors of future injury.
- Post-rehab runners require progressive return-to-run protocols and ongoing maintenance.
6. Simplify running injury prevention Messaging
Instead of overwhelming runners with multiple strategies, educate prevention around three aspects:
Load. Strength. Recovery.
If those are managed consistently, most other variables become secondary.
Regular running assessments, go a long way in proper monitoring of running mechanics. Using technology not only reduces inter-rater bias, but also makes it easy for runners to understand issues and be more compliant. GaitON offers a running assessment module to analyse running mechanics to identify movement-related risk factors for RRIs. Feel free to contact us for a demo!
ABOUT THE AUTHOR

GAYATRI SURESH (PT)
Gayatri Suresh (PT) is a Biomechanist who has completed her B.P.Th from DES College of Physiotherapy and M.P.T (Biomechanics) from SRM College of Physiotherapy, SRMIST. Her field of clinical expertise is in movement assessments through video analysis. Apart from her work at Auptimo, she works as a Clinical Specialist at Rehabilitation Research and Device Development, IIT Madras. She has won gold medals for her Research presentations and for securing First rank with distinction in her MPT degree respectively.
References
For injury incidence, prevalence types and etiology
- van Gent RN, Siem D, van Middelkoop M, van Os AG, Bierma-Zeinstra SM, Koes BW. Incidence and determinants of lower extremity running injuries in long distance runners: a systematic review. Br J Sports Med. 2007 Aug;41(8):469-80.
- Buist I, Bredeweg SW, Bessem B, van Mechelen W, Lemmink KA, Diercks RL. Incidence and risk factors of running-related injuries during preparation for a 4-mile recreational running event. Br J Sports Med. 2010 Jun;44(8):598-604.
- Linton L, Valentin S. Running with injury: A study of UK novice and recreational runners and factors associated with running related injury. J Sci Med Sport. 2018 Dec;21(12):1221-1225.
- Kakouris N, Yener N, Fong DTP. A systematic review of running-related musculoskeletal injuries in runners. J Sport Health Sci. 2021 Sep;10(5):513-522.
- Gomes Neto, M., Fossati Metsavaht, L., Luciano Arcanjo, F. et al. Epidemiology of Lower-extremity Musculoskeletal Injuries in Runners: An Overview of Systematic Reviews. Curr Emerg Hosp Med Rep 11, 74–87 (2023).
For injury prevention strategies
- Vincent HK, Brownstein M, Vincent KR. Injury Prevention, Safe Training Techniques, Rehabilitation, and Return to Sport in Trail Runners. Arthrosc Sports Med Rehabil. 2022 Jan 28;4(1)
- Linton L, Culpan J, Lane J. Running-Centred Injury Prevention Support: A Scoping Review on Current Injury Risk Reduction Practices for Runners. Transl Sports Med. 2025 Feb 25;2025:3007544.
- Johnston CA, Taunton JE, Lloyd-Smith DR, McKenzie DC. Preventing running injuries. Practical approach for family doctors. Can Fam Physician. 2003 Sep;49:1101-9.
Commentary on why injury rates are not reducing
The information found within this site is for general information only and should not be treated as a substitute for professional advice from a licensed medical practitioner. Any application of exercises and diagnostic tests suggested is at the reader’s sole discretion and risk.