Running is one of the most popular forms of physical activity around the world. Yet, prevalence of running biomechanics
related injuries remain high in spite of advancement in coaching practices, running shoes and running practices.
The most common pathologies faced by runners are Achilles tendinopathy, Calf strain, Medial Tibial Stress Syndrome, Patellar Tendinopathy and Hamstring strain.
Running biomechanics related injuries are multifactorial – ranging from non-modifiable factors such as gender, previous injuries, unforeseen events to modifiable factors such as running shoes, movement patterns, training loads, anthropometry and running surface.
While these injuries cannot be prevented altogether, here are some running biomechanics errors that can be addressed to reduce the risk of injuries.
Common running biomechanics errors
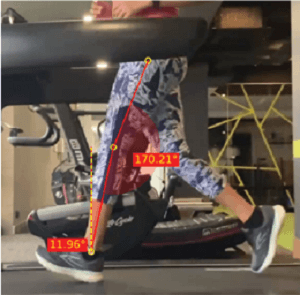
1. Overstriding + Low Cadence
|
How It Looks |
Why It Matters |
What It Often Reflects |
Corrections |
|
Foot lands well ahead of COM |
Higher peak braking forces prospectively linked to injury risk |
Long-stride preferred pattern |
Cadence retraining (+5–10%) |
|
Knee extended at contact |
+5–10% cadence reduces PFJ load & braking forces |
Quad-dominant mechanics |
Hip + knee extensor strengthening |
|
Cadence <160–165 spm |
Shorter step length reduces knee joint stress |
Underuse of hip extensors |
Cues: “Land under hips”, “Quicker steps” |
|
Education on reducing braking rather than “fixing heel strike” |
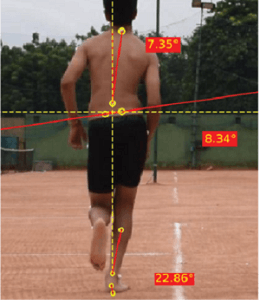
2. Dynamic Knee Valgus / Hip Adduction / Pelvic Drop
|
How It Looks |
Why It Matters |
What It Often Reflects |
Corrections |
|
Knee collapses medially |
Increased hip adduction & pelvic drop seen in PFPS |
Low hip abductor capacity |
Hip abductor strengthening |
|
Contralateral pelvic drop |
Hip abductor strengthening reduces pelvic drop (RCTs) |
Impaired single-leg control |
Frontal-plane gait retraining |
|
Narrow step width or “crossover” |
Predictive of injury in female runners |
Narrow step width |
Step width adjustment
|
|
|
|
|
Cues: “Run on train tracks”, “Keep pelvis level” |
3. High-Impact / “Loud” Landing
|
How It Looks |
Why It Matters |
What It Often Reflects |
Corrections |
|
Audible foot slap |
Higher loading rates associated with MTSS & tibial stress fractures |
Overstriding |
Impact gait retraining (auditory/visual feedback) |
|
Large vertical impact peak |
Impact-focused gait retraining reduces tibial shock |
Stiff ankle strategy |
Cadence increase |
|
High tibial acceleration |
Lowering impact does not worsen running economy |
Reduced shock absorption
|
Calf–soleus strengthening (especially bent-knee raises) |
|
|
|
Low tissue capacity |
Cues: “Run quietly”, “Soft landings” |
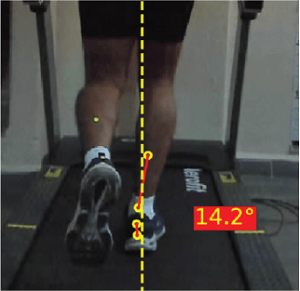
4. Narrow Step Width / Crossover Gait
|
How It Looks |
Why It Matters |
What It Often Reflects |
Corrections |
|
Feet land on or across midline |
Narrow width increases hip adduction and pelvic drop |
Motor strategy habit (often seen in novice runners) |
Step width increase (5–8 cm wider) |
|
Feet land on or across midline |
Higher ITB strain and greater tibial bending stress |
Low frontal-plane hip stability |
Mirror feedback to reduce crossover |
|
|
Linked to PFPS and lateral hip pain |
|
Hip abductor Strengthening
|
|
|
|
|
Cues: “Land under the same-side hip” |
5. Excessive Pronation / Medial Foot Collapse
|
How It Looks |
Why It Matters |
What It Often Reflects |
Corrections |
|
Midfoot cllapses medially |
Excessive pronation associated with MTSS, plantar fasciopathy & tibial rotation stress |
Medial arch weakness |
Foot intrinsic strengthening (short-foot, toe-mobility drills) |
|
Tibial internal rotation visibly increases |
Greater foot mobility correlates with higher injury incidence |
Reduced tibialis posterior capacity |
Tibialis posterior strengthening |
|
Arch height drops under load |
|
Foot-intrinsic weakness |
Step width or cadence modifications to reduce medial load |
|
|
|
|
Footwear guidance (not as a primary fix) |
6. Pelvic Over-Rotation / Excessive Trunk Rotation
|
How It Looks |
Why It Matters |
What It Often Reflects |
Corrections |
|
Arms cross midline |
Increases shear at spine & pelvis |
Low trunk control |
Anti-rotation training (Pallof press, carries) |
|
Torso rotates excessively |
Associated with low back pain in runners |
Weak obliques and deep stabilisers |
Cueing: “Arms forward-back, not side-to-side” |
|
Lower limb “scissor pattern” |
Often coexists with asymmetrical hip mechanics |
Crossover gait |
Widen step width |
|
|
|
|
Strengthening glutes/rotational control |
7. Late Heel Lift / Limited Ankle Stiffness
|
How It Looks |
Why It Matters |
What It Often Reflects |
Corrections |
|
Heel stays on the ground longer than ideal |
Reduced ankle stiffness reduces running economy |
Weak plantar flexors (especially soleus) |
Soleus-dominant strengthening (bent-knee calf raise progressions) |
|
Low vertical stiffness |
Associated with calf–Achilles overload due to compensatory propulsion patterns |
Limited ankle stiffness during midstance |
Plyometrics (pogo jumps, hops) to increase ankle stiffness |
|
Knee stays flexed too long |
|
|
Cadence increase to reduce overloading |
|
|
|||
The easiest way to assess and identify all these biomechanical issues is through a running gait analysis. Modern day technology now offers portable, accurate and cost-effective solutions for running analysis. To launch running analysis at your center, contact us today!
ABOUT THE AUTHOR

GAYATRI SURESH (PT)
Gayatri Suresh (PT) is a Biomechanist who has completed her B.P.Th from DES College of Physiotherapy and M.P.T (Biomechanics) from SRM College of Physiotherapy, SRMIST. Her field of clinical expertise is in movement assessments through video analysis. Apart from her work at Auptimo, she works as a Clinical Specialist at Rehabilitation Research and Device Development, IIT Madras. She has won gold medals for her Research presentations and for securing First rank with distinction in her MPT degree respectively.
References for common running biomechanics errors
- Heiderscheit BC et al. Effects of step rate manipulation on joint mechanics during running. Med Sci Sports Exerc. 2011.
- Lenhart RL et al. Increasing running step rate reduces patellofemoral joint forces. Med Sci Sports Exerc. 2014.
- Willy RW, Davis IS. The effect of a hip strengthening program on mechanics and pain in females with PFPS. J Orthop Sports Phys Ther. 2011.
- Napier C, MacLean CL, Maurer J, Taunton JE, Hunt MA. Kinetic risk factors of running-related injuries in female recreational runners. Scand J Med Sci Sports. 2018
- Noehren B, Hamill J, Davis I. Prospective evidence for a hip etiology in patellofemoral pain. Med Sci Sports Exerc. 2013
- Souza RB, Powers CM. Differences in hip kinematics, muscle strength, and muscle activation between subjects with and without patellofemoral pain. J Orthop Sports Phys Ther. 2009
- Crowell HP, Davis IS. Gait retraining to reduce lower extremity loading in runners. Clin Biomech (Bristol). 2011
- Winkelmann ZK, Anderson D, Games KE, Eberman LE. Risk Factors for Medial Tibial Stress Syndrome in Active Individuals: An Evidence-Based Review. J Athl Train. 2016
- Meardon SA, Campbell S, Derrick TR. Step width alters iliotibial band strain during running. Sports Biomech. 2012
- Bramah C, Preece SJ, Gill N, Herrington L. Kinematic Characteristics of Male Runners With a History of Recurrent Calf Muscle Strain Injury. Int J Sports Phys Ther. 2021
The information found within this site is for general information only and should not be treated as a substitute for professional advice from a licensed medical practitioner. Any application of exercises and diagnostic tests suggested is at the reader’s sole discretion and risk.