With an injury rate of 2.35 per 1000 in the adult population (de Jonge et all, 2011), the Achilles tendon is one of the most commonly injured tendons, especially in athletes involved in running and jumping sports/activities (Kvist, 1994) (Wilson, 2005)
As per studies, the loading on the Achilles tendon during running increases to 12 times the body weight. This is much higher as compared to walking (upto 3.5 times body weight), or cycling (close to body weight) (Komi, et al., 1992). Such loading rates when combined with improper running biomechanics can be detrimental to Midportion Achilles Tendinopathy issues in runners.
A gait analysis, whether observational or through a video based system, is an excellent way to identify any biomechanical faults in the runner. A biomechanical fault can be as a result of either a physical limitation in the body or a technical error in the running form.
In this blog, we will discuss various biomechanical faults that are associate with excessive loading on the Achilles tendon.
BIOMECHANICAL FAULTS ASSOCIATED WITH INCREASED ACHILLES LOADING
FOOT STRIKE PATTERN
Running with a rear footstrike pattern is considered to load the Achilles tendon less than running with a forefoot-strike pattern (Komi, et al., 1992). As per recent studies, running with a midfoot- or forefoot-strike pattern, as opposed to a rearfoot-strike pattern, added an additional load of 48 times body weight for each mile (1.6 km) run. (Almonroeder, et al., 2013)
ASSESSMENT OF FOOT STRIKE PATTERN
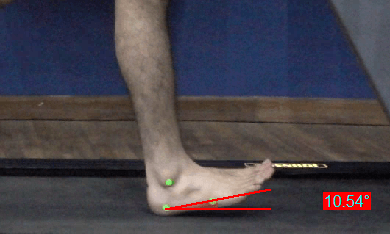
Foot strike pattern can be determined by measuring the foot inclination angle.
The foot inclination angle is the angle between the running surface and the sole of the runner’s shoe and allows for the determination of foot-strike pattern.
Heel strike
(Landing on the posterior aspect of their heel)
Rearfoot strike
(Landing on the anterior aspect of the heel, with FIA <10 degrees)
Midfoot strike
(Rearfoot & forefoot making contact nearly simultaneously, with FIA near 0°)
Forefoot strike
(Forefoot landing with FIA <0 degrees)
Within the context of return to sport, to control for overall loading, a runner who runs with a forefoot-strike pattern would not be allowed to run as far as a runner with a rearfoot-strike pattern. (SILBERNAGEL & CROSSLEY, 2015)
OVERSTRIDING
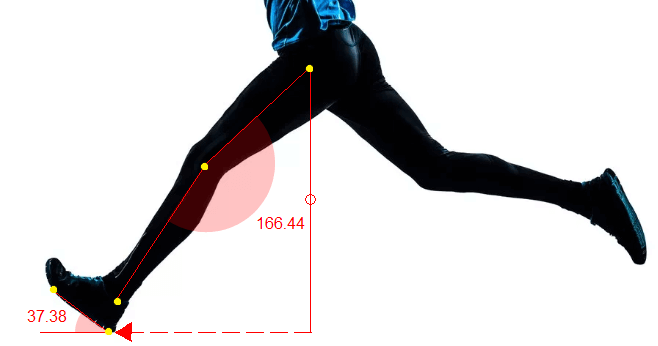
Overstriding can be picked up when reviewing the video taken in the sagittal plane.
The term simply means that the runner is landing excessively ahead of the center of mass of the body (COM can be approximated at the center of the pelvis). Doing this often increases the stride length of the runner, hence the name ‘overstriding’. (Souza, 2016 )
OVERPRONATION
Recent studies have linked excessive subtalar eversion with excessive Midportion Achilles Tendinopathy. In a study comparing running mechanics of runners with Achilles Mid-Portion Tendinopathy with healthy runners, The Achilles Tendinopathy Group displayed significantly greater sub-talar joint eversion displacement during mid-stance of the running gait. (Ryan M, 2009)
Exercise programs for arch strengthening etc along with foot orthotics can be helpful in reducing excessive calcaneal eversion and reducing the load on Achilles tendon loading.
ASSESSMENT OF SUBTALAR EVERSION
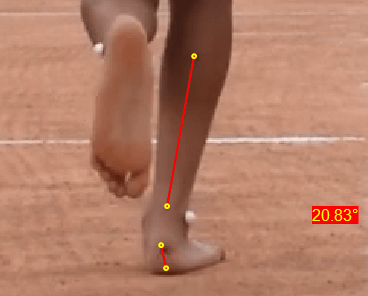
Subtalar eversion can be assessed by measuring the rearfoot angle in the posterior view. Rearfoot angle is defined by the midline of the heel relative to the midline of the lower leg.
Any running gait analysis software like GaitON can be used to do a comprehensive running analysis of the runner. All you need is the software and the slow motion video feature of your mobile phone to start.
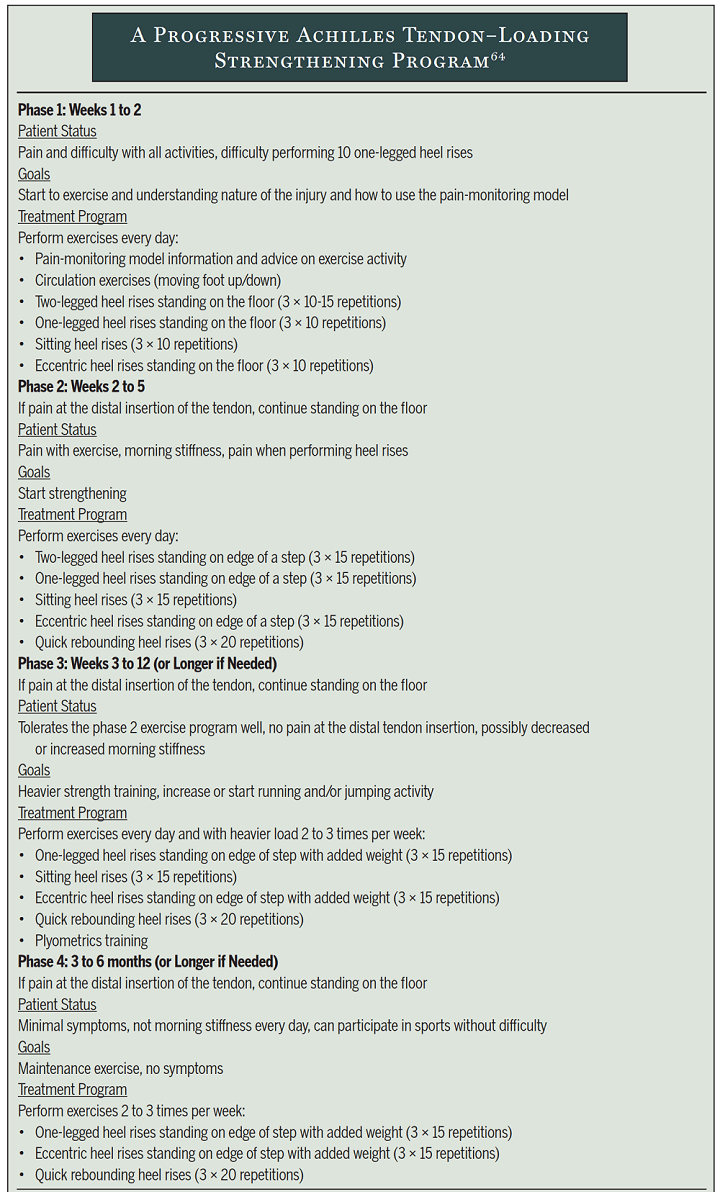
EXERCISE AS A TREATMENT
Exercise therapy is consistently supported with the highest level of evidence, and eccentric exercise is the most investigated type of exercise therapy. (Kingma, et al., 2007) It is recommended to initially treat all patients with exercise therapy for at least 3 months prior to considering other treatment options. (Alfredson, 2003).
Mentioned below is a progressive Achilles tendon–loading strengthening program that promotes exercise once daily and uses concentric/eccentric exercises.