Running is a wildly popular sport. It is a great form of exercise for both body and mind and it can be done almost anywhere – all you need is a comfortable pair of sneakers. Unfortunately, this sudden increase in running has also led to an exponential increase in running related injuries.
As physiotherapists, this is where we come in. From strength training to stretching to foam rolling, we use different techniques to keep injuries it bay. But lets face it. We all know that runners can be tricky patients. We can do everything right with them, but they still manage to find a way to get that pain back. Are we missing something?
We haven’t watched them run! What our injured runners really need is gait retraining.
Having a good understanding of joint motion and biomechanics, physical therapists are well suited to help runners improve their form. Improving running form can mean two things.
First would be to eliminate any physical limitation in the body(a tight calf, a weak ligament etc.). The other factor would be improving running technique (increased step length, reduced cadence etc.) to eliminate any bio-mechanical fault that may lead to injuries. Incorporating these methods of gait retraining into our practice with runners will not only help our patients recover from injury faster, but it will also allow them to run more efficiently. Your runners will be eternally grateful for your expertise.
To get a better understanding of gait, you can shoot videos from different views. Typically, videos from posterior, lateral and the anterior views are required. While recording, ensure that the runners's entire body is in the frame.
Your next step is to review the video with the patient. From personal experience, runners would really appreciate this. It is helpful for them to see what they look like running. The individualized approach makes it more likely that they will remember your advice and also buy into your treatment plan. Just make sure to avoid PT jargon in your explanation (i.e. dynamic knee valgus, pelvic drop etc.)
Running form evaluation
Since we don’t always have much time in the clinic, I will be talking about the major issues that you will find in a number of runners. First in that list is ‘Overstriding’. This is a fault that will be present in 60–70% of runners that visit you, especially novice runners. Here is how you can detect if a patient is overstriding.
#Theoverstriders
Overstriding can be picked up when reviewing the video taken in the sagittal plane. The term simply means that the runner is landing excessively ahead of the center of mass of the body(COM can be approximated at the center of the pelvis). Doing this often increases the stride length of the runner, hence the name ‘overstriding’.
This may sound efficient, but overstriding has been linked to a variety of running injuries including patellofemoral pain syndrome, iliotibial band syndrome, plantar fasciitis, achilles tendonitis and tibial stress fractures.
These injuries often result from excessive impact forces at the hip, knee and ankle joints, which accompany overstriding.
When examining video in the lateral view, there are several key elements that will alert you about overstriding. These include any combination of the following:
- Increased vertical excursion of the center of mass(COM)
- Reduced knee flexion angle at foot strike
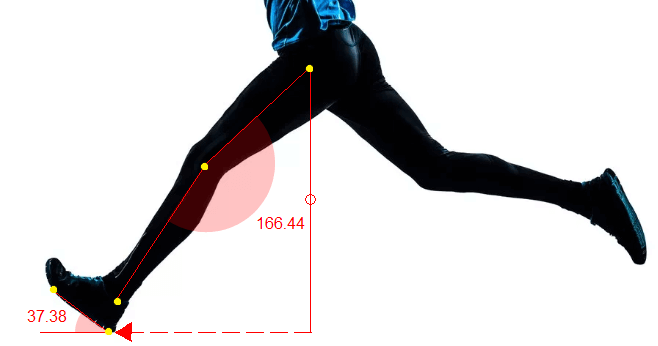
- Increased foot inclination angle foot strike
- Excessive horizontal distance between foot and COM at foot strike
Below is an example of an overstrider. In this photo you can clearly see that upon initial contact, the knee is almost fully extended and the foot exhibits a large foot inclination angle.
Runners with overstriding fault benefit from gait retraining that targets shortening stride length and increasing step rate. By simply taking more steps and therefore decreasing their stride length, the impact ground reaction forces can be decreased. This improve the chances of injury recovery and future injury prevention.
Cadence retraining
If a runner can learn to increase their step rate, their stride will shorten and the resultant impact forces will decrease. There is no magic number for step rate – it simply has to be higher than the runner’s originally preferred step rate. Increases as little as 5% have been shown to reduce joint compression forces and decrease risk of injury. This alteration in running mechanics has proven to be just as, if not more important, than a strengthening program.
There are several ways that we can help a runner increase step rate. Runners can use a metronome app to match their steps to a desired step rate, but they can also use their playlist to achieve this.
If used properly, a running evaluation can be a very valuable to your practice. It helps you understand how a physical limitation (e.g. flat feet) in the runner effects the entire body. Using tools like motion analysis software can increase the accuracy of this entire process by giving you a complete breakdown of the runner’s mechanics during the entire gait cycle.
After interacting with hundreds of clinicians, we crafted the running analysis protocol of GaitON with an aim to analyse a runner’s gait more effectively and easily. The protocol helps a clinician analyse the pelvis, hip, knee, foot and ankle joint motion during the running gait cycle. All the data is then well documented to a report with reference values! Click here to know more.