“But how can the quadriceps be ‘avoided’ in Gait?” A “quadriceps avoidance gait” is a pathological gait pattern in which a person may consciously or subconsciously avoid quadriceps usage in gait.
POTENTIAL CAUSES OF QUADRICEPS AVOIDANCE GAIT
The causes for such a gait may be –
- Pain or Injury: If it’s specific to the quadriceps, a person might change their gait to reduce contraction to prevent discomfort.
- Weakness: Weakness in the quadriceps muscles, whether due to injury, neuromuscular conditions, or disuse, can lead to a compensatory gait pattern. The person may adopt a gait that relies more on other muscle groups to compensate for the weakness.
- Neurological Conditions: Certain neurological conditions, such as stroke or nerve damage, can affect the ability to control the quadriceps muscles properly. This can result in an altered gait pattern where the individual struggles to fully extend their knee during walking. Typical presentations such as hand-to-knee gait, hyperextension during loading response and trunk flexion during midstance are seen in these conditions.
- Muscle Imbalances: Muscle imbalances in the lower extremities can also lead to a quadriceps avoidance gait. For example, if the hamstrings are significantly stronger than the quadriceps, it can lead to an altered gait pattern.
- Surgical Procedures: Some individuals may develop a quadriceps avoidance gait after knee surgery or procedures that affect the quadriceps tendon or the joint mechanics.
- Compensatory Mechanism: In some cases, the gait can be a compensatory mechanism for another issue, such as hip pain or instability.
ROLE OF QUADRICEPS DURING GAIT
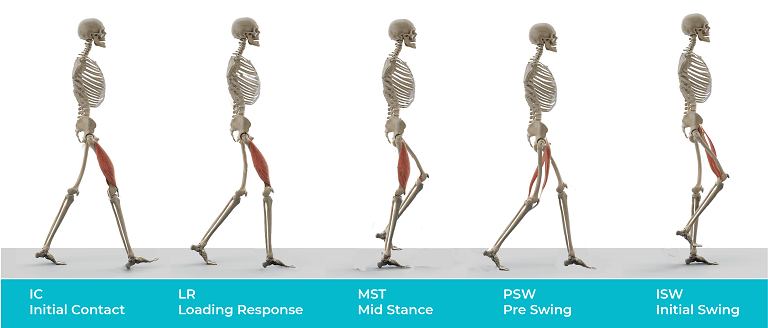
Fig. 1: Gait cycle phases with increased quadriceps muscle activity
- Initial Contact – Eccentric Contraction to provide a controlled knee flexion
- Loading response – Concentric Contraction to provide knee extension
- Pre-swing – Eccentric contraction to provide a controlled knee flexion (Rectus Femoris)
- Early swing – Eccentric Contraction to provide a controlled knee flexion (Rectus Femoris)
CASE BACKGROUND
We had a client come in for gait analysis, and incidentally, she demonstrated a Quadriceps Avoidance Gait Pattern. In this article, we explore her kinematic gait analysis, the potential causes for the gait, and a suitable rehabilitation plan.
I. Demographic Details
Age (years) | 53 |
Gender | Female |
Weight (Kgs) | 61 |
Height (cm) | 155 |
Chief Complaint | Right knee pain and knee buckling |
Clinical Observations | Right patellar instability and patellofemoral pain syndrome, Reduced Right medial arch |
II. Gait Analysis setup to assess quadriceps avoidance gait

Fig. 2 The figure shows a treadmill-based gait analysis setup used for the analysis consisting of 4 cameras (1 each for left lateral view, right lateral view, anterior and posterior view).
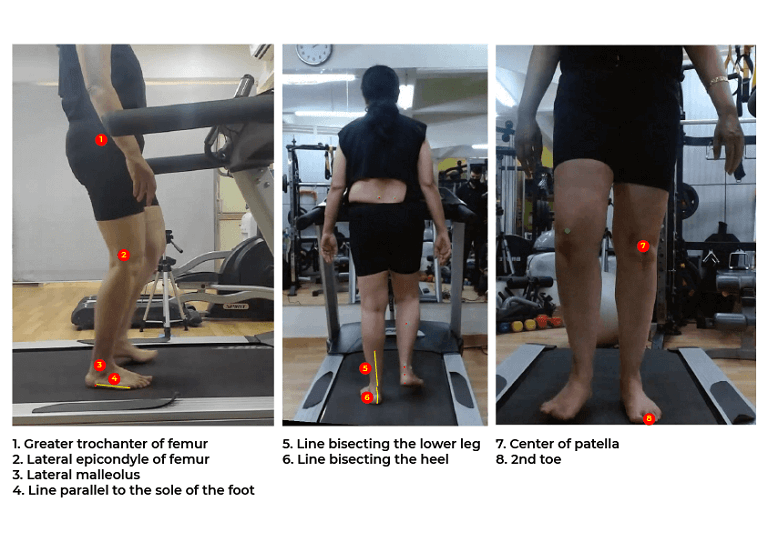
Fig. 3 showing the surface landmarks used for placing self-adhesive markers for joint angle calculation. A tight-fitting t-shirt and shorts was used to ensure minimal marker movement.
III. Joint Angles to assess quadriceps avoidance gait
Angle Name | Definition |
Hip Angle (Flexion/Extension) | Angle created by Greater trochanter of femur , Lateral epicondyle of femur with the vertical |
Knee Angle (Flexion/Extension) | Angle created by Greater trochanter of femur , Lateral epicondyle of femur and Lateral malleolus |
Ankle Angle (Dorsiflexion/Plantar flexion) | Angle created by Lateral epicondyle of femur, Lateral malleolus and a line parallel to sole of foot |
Pelvic Drop (Contralateral/ipsilateral pelvic drop or hip hiking) | Angle created by a line joining the PSIS’s with the horizontal |
Rearfoot Angle (Eversion/Inversion) | Angle created by the lines bisecting the lower leg and heel |
Knee abduction/Adduction | Angle created by a center of patella, 2nd toe with vertical. |
KINEMATIC ANALYSIS : QUADRICEPS AVOIDANCE GAIT
The phases are described as per RLA classification
Stance Phase
a. Joint angles at Initial Contact
Joint | Angle (Left) | Angle (Right) | Normal values | Interpretation |
Hip | (+) 24.9° | (+) 20.1° | (+) 20° to (+) 27° | Normal ranges |
Knee | 175.2° | 176.2° | 168° to 178° | Normal ranges |
Ankle | 104.8° | 103.5° | 90° to 95° | Increased plantarflexion at both ankle joints |
(+) : Hip Flexion, (-) : Hip Extension, Knee hyperextension (Angle > 180), Knee flexion (Angle< 180), Ankle Plantarflexion (Angle > 90), Ankle Dorsiflexion (Angle< 90)
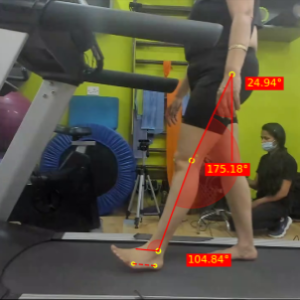
Fig. 4a – Joint angles of Left Hip, Knee and Ankles at Left Initial Contact
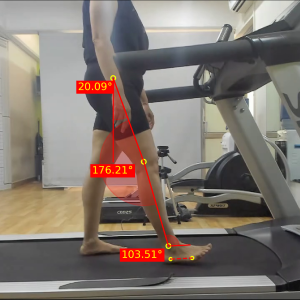
Fig. 4b – Joint angles of Right Hip, Knee and Ankles at Right Initial Contact
This phase of gait did not show a major deviation in the knee angles. Although, both ankle joints were plantarflexed more than necessary, which may be indicative of reduced eccentric control of the dorsiflexors (Bilateral)
b. Joint angles at end of Loading response
Joint | Angle (Left) | Angle (Right) | Normal Values | Interpretation |
Hip | (+) 19.4° | (+) 17.8° | (+) 19° to (+) 26° | Slightly increased hip extension of right hip |
Knee | 164.6° | 151.4° | 156° to 165° | Increase in right knee flexion |
Ankle | 101.5° | 81.4° | 90° to 96° | Increased plantarflexion at left ankle
Increased dorsiflexion at the right ankle |
(+) : Hip Flexion, (-) : Hip Extension, Knee hyperextension (Angle > 180), Knee flexion (Angle< 180), Ankle Plantarflexion (Angle > 90), Ankle Dorsiflexion (Angle< 90)
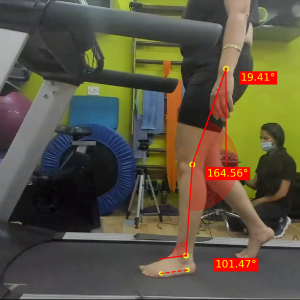
Fig. 5a – Joint angles of Left Hip, Knee and Ankles at Left Loading Response
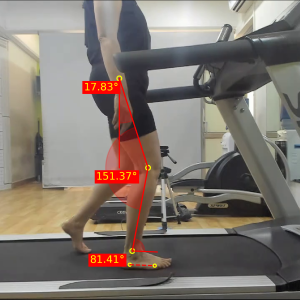
Fig. 5b – Joint angles of Right Hip, Knee and Ankles at Right Loading Response
In this phase, we start seeing compensatory changes. An increased right knee flexion (‘knee buckle’) indicates reduced eccentric contraction force by the quadriceps. This increase in knee flexion also causes an increase in dorsiflexion at the right ankle. Even though changes are present, this phase is not fully indicative of a quadriceps avoidance gait.
Further, an increased left ankle plantarflexion may be indicative of reduced eccentric control of the dorsiflexors.
c. Joint angles at end of Mid Stance
Joint | Angle (Left) | Angle (Right) | Normal Values | Interpretation |
Hip | (+) 7.2° | (+) 11.2° | 0° to (-) 6° | Increased flexion at left and right hip |
Knee | 171.8° | 151.6° | 168° to 177° | Increased right knee flexion |
Ankle | 96.9° | 76.7° | 78° to 86° | Increased plantarflexion at left ankle
Increased dorsiflexion at the right ankle |
(+) : Hip Flexion, (-) : Hip Extension, Knee hyperextension (Angle > 180), Knee flexion (Angle< 180), Ankle Plantarflexion (Angle > 90), Ankle Dorsiflexion (Angle< 90)
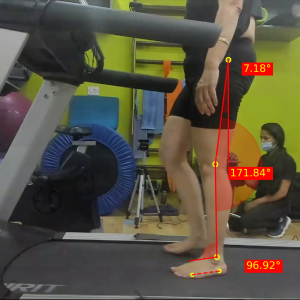
Fig. 6a – Joint angles of Left Hip, Knee and Ankles at Left Mid Stance
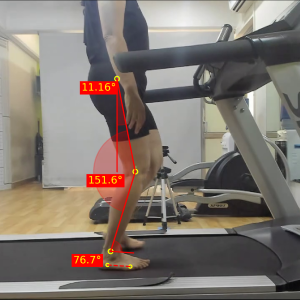
Fig. 6b – Joint angles of Right Hip, Knee and Ankles at Right Mid Stance
This phase shows a clear increase in right knee flexion, with the knee being approximately 20 degrees more flexed than the left. Consequently, this excessive knee flexion reduces the effective leg length of the right limb and reduces ground clearance for the left limb to swing forward.
The increased right knee flexion also causes a delay in hip extension, which should have reached neutral. The flexion also results in an increased ankle dorsiflexion.
Further, an increased left ankle plantarflexion may be indicative of increased tightness of the plantarflexors.
1. Joint angles at end of Mid Stance: Frontal Plane
Component | Angle (Left) | Angle (Right) | Normal Values | Interpretation |
Pelvic Drop* | (+) 2.5° | (-) 3.1° | 0° to (+) 5° | Pelvic hike at right mid stance |
Knee abd/add** | (+) 2.3° | (+) 4.1° | 0° | Increased medial tracking of both patellae, Right> Left |
Rear foot angle*** | (+) 8.1° | (+) 11.4° | (+) 2° to (+) 6° | Increased rear-foot eversion at both feet, Right > Left |
*(+) : Contralateral Pelvic Drop (-) : Ipsilateral pelvic drop, **(+): Knee Abduction, (-): Knee Adduction, ***(+) Eversion, (-) Inversion
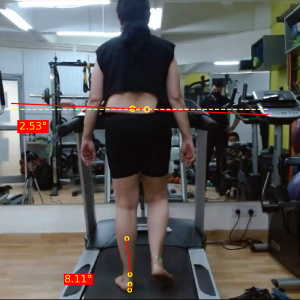
Fig. 7a – Posterior view joint angles at Left Mid Stance
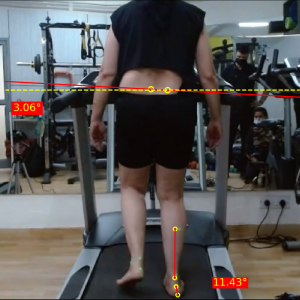
Fig. 7b – Posterior view joint angles at Right Mid Stance

Fig. 8a – Anterior view joint angles at Left Mid Stance

Fig. 8b – Anterior view joint angles at Right Mid Stance
Posteriorly, a left-sided hip hike is seen during right midstance, indicating a compensatory hike to clear the ground due to the shorted right limb resulting from an increased knee flexion.
While an increased foot pronation (eversion) is seen the likely cause is the client’s posture, rather than the knee pathology (Bilateral).
The increased medial tracking of the right patella could be explained by the increased rearfoot eversion and increased knee flexion at mid stance.
d. Joint angles at end of Terminal Stance
Joint | Angle (Left) | Angle (Right) | Normal Values | Interpretation |
Hip | (-) 5.7° | (-) 6.4° | (-) 15° to (-) 23° | Reduced extension at left and right hip |
Knee | 180.0° | 168.6° | 163° to 171° | Increased extension at left knee |
Ankle | 93.1° | 80.4° | 76° to 84° | Increased plantarflexion at left ankle |
(+) : Hip Flexion, (-) : Hip Extension, Knee hyperextension (Angle > 180), Knee flexion (Angle< 180), Ankle Plantarflexion (Angle > 90), Ankle Dorsiflexion (Angle< 90)

Fig. 9a – Joint angles of Left Hip, Knee and Ankles at Left Terminal Stance
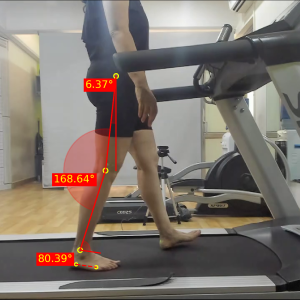
Fig. 9b – Joint angles of Right Hip, Knee and Ankles at Right Terminal Stance
An increased left ankle plantarflexion may be indicative of increased tightness of the plantarflexors. Furthermore, as seen in previous phases of gait cycle, the hip extends less than normal (Bilateral)
e. Joint angles at end of Pre Swing
Joint | Angle (Left) | Angle (Right) | Normal Values | Interpretation |
Hip | (+) 3.0° | (+) 1.4° | (-) 7° to (-) 15° | Reduced extension at left and right hip |
Knee | 139.4° | 135.7° | 136° to 147° | Slightly increased flexion at right knee |
Ankle | 119.6° | 103.3° | 99° to 109° | Increased plantarflexion at left ankle |
(+) : Hip Flexion, (-) : Hip Extension, Knee hyperextension (Angle > 180), Knee flexion (Angle< 180), Ankle Plantarflexion (Angle > 90), Ankle Dorsiflexion (Angle< 90)
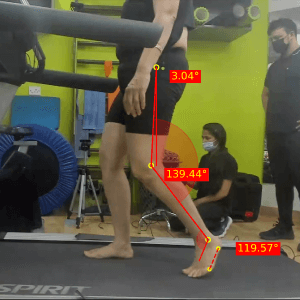
Fig. 10a – Joint angles of Left Hip, Knee and Ankles at Left Pre Swing

Fig. 10b – Joint angles of Right Hip, Knee and Ankles at Right Pre Swing
The increased knee right flexion in this phase is another indication of the reduced power of right quadriceps which are supposed to act eccentrically to control the knee flexion provided by the vertical ground reaction forces that pass posteriorly to the knee joint during pre-swing. Further, an increased left ankle plantarflexion may be indicative of increased tightness of the plantarflexors.
Swing Phase
a. Joint angles at end of Initial Swing
Joint | Angle (Left) | Angle (Right) | Normal Values | Interpretation |
Hip | (+) 22.4° | (+) 22.2° | (+) 9° to (+) 17° | Increased flexion at left and right hips |
Knee | 140.6° | 135.4° | 116° to 126° | Reduced flexion at left and right knees |
Ankle | 112.7° | 94.1° | 94° to 104° | Increased plantarflexion at left ankle |
(+) : Hip Flexion, (-) : Hip Extension, Knee hyperextension (Angle > 180), Knee flexion (Angle< 180), Ankle Plantarflexion (Angle > 90), Ankle Dorsiflexion (Angle< 90)

Fig. 11a – Joint angles of Left Hip, Knee and Ankles at Left Initial Swing
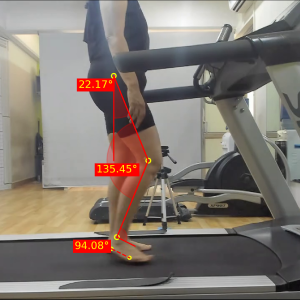
Fig. 11b – Joint angles of Right Hip, Knee and Ankles at Right Initial Swing
A common consequence of painful gait is reduced peak knee flexion at the end of initial swing, which is seen in this case. Additionally, an increased left ankle plantarflexion may be indicative of reduced concentric activity of the dorsiflexors.
b. Joint angles at end of Mid Swing
|
Joint |
Angle (Left) |
Angle (Right) |
Normal Values |
Interpretation |
|
Hip |
(+) 22.6° |
(+) 22.2° |
(+) 22° to (+) 30° |
Within Normal ranges |
|
Knee |
155.8° |
156.7° |
146° to 157° |
Within Normal ranges |
|
Ankle |
110.7° |
95.3° |
87° to 93° |
Increased plantarflexion at left and right ankles |
(+) : Hip Flexion, (-) : Hip Extension, Knee hyperextension (Angle > 180), Knee flexion (Angle< 180), Ankle Plantarflexion (Angle > 90), Ankle Dorsiflexion (Angle< 90)

Fig. 12a – Joint angles of Left Hip, Knee and Ankles at Left Mid Swing
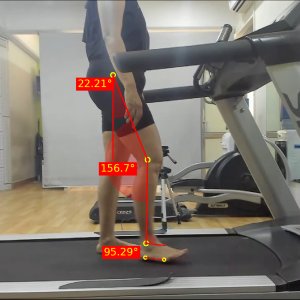
Fig. 12b – Joint angles of Right Hip, Knee and Ankles at Right Mid Swing
Due to absence of any ground reaction forces in the swing, the effect of quadriceps avoidance is generally not seen during the swing phases. Moreover, an increased left ankle plantarflexion may be indicative of reduced concentric activity of the dorsiflexors.
DISCUSSION : QUADRICEPS AVOIDANCE GAIT
The client demonstrates a right-sided quadriceps avoidance gait.
She has previously been diagnosed with Patellofemoral Pain Syndrome (PFPS).
While the specific diagnosis is not known, a plausible theory for her pathological gait pattern would be anterior instability.
Since it’s a well-known fact that knee extension is a loose pack position for the patellofemoral joint, the client may have subconsciously avoided terminal knee extension over a period of time.
Postural deviations of increased knee valgus and foot pronation are seen in the frontal plane. This raises a second theory of the PFPS arising from biomechanical changes in the foot, knee and hip.
Lastly, an overall reduced hip ROM (flexion and extension) along with increased left ankle plantarflexion os also observed during the gait cycle.
The first signs of quadriceps avoidance are seen in the loading response, where an early and increased knee flexion occurs. Furthermore, a very significant increase in right knee flexion is seen during mid-stance. Wherein the degree of flexion should be around 7 degrees, it is flexed by 30 degrees.
The evidence pertaining to gait deviations in patellofemoral pathology is limited but mostly shows an overall increase in knee flexion during stance phases and a reduction in knee flexion during the swing phases of gait. [1], [2]
These compensations occur to reduce discomfort and instability during terminal extension and reduce compressive forces during flexion, respectively.
Rehabilitation Goals
- Pain/discomfort Reduction
- Quadriceps strengthening in open and closed kinematic chain
- Proprioceptive training
- Posture correction
- Single limb progressive loading
- Strengthening of proximal and distal muscles
What management would you suggest for this gait?
Do drop your thoughts in the comments!
We hope that this blog helped you get a clear understanding of abnormal gait patterns in quadriceps avoidance gait.
Setting up your own gait analysis lab is now easier than ever. To learn more about GaitON’s gait analysis modules, contact us today!
Since you’re here…
…we have a small favor to ask. More people are reading our blogs everyday, and each week we bring you compelling content to help you treat your patients better. Please take a moment to share the articles on social media, engage the authors with questions and comments below, and link to articles when appropriate if you have a blog or participate on forums of related topics. — Team Auptimo
The information found within this site is for general information only and should not be treated as a substitute for professional advice from a licensed Physiotherapist. Any application of exercises and diagnostic tests suggested is at the reader’s sole discretion and risk.
ABOUT THE AUTHOR
GAYATRI SURESH (PT)
Gayatri Suresh (PT) is a Biomechanist who has completed her B.P.Th from DES College of Physiotherapy and M.P.T (Biomechanics) from SRM College of Physiotherapy, SRMIST. Her field of clinical expertise is in movement assessments through video analysis. Apart from her work at Auptimo, she works as a Clinical Specialist at Rehabilitation Research and Device Development, IIT Madras. She has been conferred with gold medals for her Research presentations and for securing First rank with distinction in her MPT degree respectively
REFERENCES (QUADRICEPS AVOIDANCE GAIT):
- Damian A. Clark, Danielle L. Simpson, Jonathan Eldridge, G. Robert Colborne, Patellar instability and quadriceps avoidance affect walking knee moments, The Knee, Volume 23, Issue 1, 2016,Pages 78-84
- Sylvie Nadeau, Denis Gravel, Luc J. Hébert, A.Bertrand Arsenault, Yves Lepage, Gait study of patients with patellofemoral pain syndrome, Gait & Posture, Volume 5, Issue 1, 1997, Pages 21-27