Gait retraining is a common area of focus in the rehabilitation of movement-related pathologies, with a primary focus on the sagittal plane — the forward-and-backward movements in running and walking. Think of cues like “take shorter steps,” “increase cadence,” or “lean forward slightly’‘ and strategies like obstacle walking, use of assistive devices, etc.
However, gait is a three-dimensional activity. Alongside the sagittal plane, which exhibits the largest joint excursion, comparatively minor but essential frontal plane and transverse plane contributions ensure a smooth and efficient gait. Compared to sagittal strategies, interventions in these planes are less common, less intuitive, and hard to measure — yet they may have equally significant effects on joint loading, injury risk, and rehab progression.
Why sagittal gait retraining strategies dominate
The reasons why sagittal-plane gait retraining is the most common:
- Easy to measure – A basic 2D video analysis or even a smartphone can capture step length, cadence, and foot strike patterns.
- Clear links to injury – High vertical impact loads and braking forces (both sagittal plane issues) are strongly associated with tibial stress fractures and patellofemoral pain.
- Simple to cue – Clients understand instructions like “increase cadence by 10%” or “bend your knee more” or “Lean a little forward”
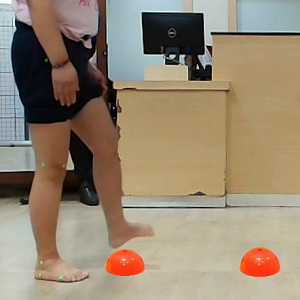
Fig: Sagittal plane gait retraining with cones being used as a way to promote greater hip and knee flexions for creating ground clearance
By contrast, frontal and transverse plane mechanics require 3D motion analysis for accuracy, and the cues are less intuitive. Asking someone to “add trunk sway” or “rotate your pelvis differently” won’t be as easy to understand as “take quicker steps.”
Hence, frontal and transverse plane gait retraining is not commonly used in clinical practice.
Why frontal and transverse planes gait retraining matters
Although the use of sagittal strategies is common, research indicates that the frontal and transverse planes play a decisive role in joint loading, pain, and long-term injury progression.
Frontal Plane: The Load Distributor
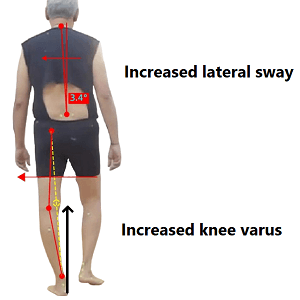
Fig: A patient using lateral trunk sway to bring the COM closer to knee joint and reduce knee adduction moment in case of a varus knee
The knee adduction moment (KAM) — a frontal plane measure — is one of the strongest predictors of medial knee osteoarthritis (OA) onset and progression. For instance, Miyazaki et al. reported that higher baseline KAM predicted a greater risk of radiographic OA progression over six years.
Furthermore, Mündermann et al. demonstrated that increasing medio-lateral trunk sway during walking reduced KAM by ~65% in healthy adults, without harmful side effects such as higher impact loading. This highlights how a simple frontal-plane cue can unload the knee joint effectively.
More recently, Uhlrich et al. conducted a randomized controlled trial showing that personalized foot progression angle retraining (toe-in or toe-out) not only reduced KAM but also slowed cartilage degradation and provided pain relief equivalent to medication. Notably, this was the first placebo-controlled trial to prove that a biomechanical intervention can alter disease progression.
Transverse Plane: The Rotational Controller
Excessive femoral internal rotation and tibial external rotation can increase patellofemoral joint stress, often associated with patellofemoral pain syndrome (PFP). Powers proposed that altered transverse-plane hip and knee mechanics are central to PFP pathophysiology.
Similarly, Noehren et al. found that female runners with PFP displayed greater hip internal rotation during running compared to controls, and that gait retraining focused on reducing hip adduction and internal rotation improved symptoms.
In addition, dynamic knee valgus — a combined frontal and transverse deviation — is also a major risk factor for ACL injury. Hewett et al. identified that athletes with poor hip and trunk control, leading to excessive valgus collapse, had significantly higher ACL injury risk. Consequently, Retraining hip rotation and trunk control has since become a key element in ACL prevention programs.
Why they matter together
- The frontal plane determines where load is distributed (medial vs. lateral compartments of the knee, hip abduction/adduction).
- The transverse plane governs how forces are directed (rotational alignment of femur, tibia, and pelvis).
Both are interconnected: for example, increased hip internal rotation (transverse) often presents alongside excessive hip adduction (frontal), together producing dynamic valgus and elevated joint stress.
Ignoring these planes risks missing the implications of joint overload and injury. While sagittal retraining reduces impact peaks, frontal and transverse retraining may directly target malalignment and rotational mechanics.
Frontal plane gait retraining strategies
1. Step Width Adjustments
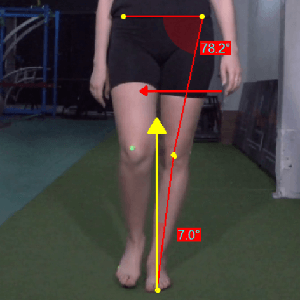
Fig: Narrow base of support, increasing hip adduction and knee adduction moments
Narrow step widths are consistently linked with higher hip adduction angles and moments, which in turn increase medial knee loading. A slight increase in step width redistributes the center of mass relative to the base of support, reducing the demand on the hip adductors and lowering medial compartment forces at the knee.
Teaching often involves visual cues, such as placing tape lines on a treadmill or floor and asking the runner to “land outside the line.” Mirror or video feedback is particularly effective to ensure the adjustment is subtle, as excessive widening may increase energy cost.
2. Foot Progression Angle (Toe-In or Toe-Out)

Fig: Role of toe-in pattern in reducing knee adduction moments
Adjusting the foot progression angle — the angle between the long axis of the foot and the line of progression — alters the line of action of the ground reaction force relative to the knee joint center. This angle directly influences the external knee adduction moment (KAM). In simple words, knee adduction moment is the ability of the ground reaction force to increase medial knee loading. KAM is directly proportional to body weight and the lateral distance between the ground reaction force (GRF) vector (which passes through center of pressure) and the knee joint center.
A toe-in gait tends to shift the center of pressure (and GRF vector) laterally under the foot in early stance. Furthermore, the knee joint center shifts medially due to internal rotation of the tibia in toe-in gait. Consequently, the distance between the GRF vector and knee joint center reduces, which also reduces the peak knee adduction moment during early stance. This strategy is minimising medial knee loading in patients with medial knee OA having an increased peak KAM during early stance.
In contrast, a toe-out gait (external foot rotation) has been observed to reduce the peak KAM during late stance. However, the peak KAM during late stance has been considered to be less correlated to the medial knee joint reaction force compared to the early stance peak during walking.
In practice, clinicians may use pressure-sensitive treadmills, gait labs, or wearable sensors to test multiple angles and select the most effective. Cueing may include “point your toes slightly inward” or “angle outward just a few degrees.”
3. Trunk Lean and Sway
Increasing medio-lateral trunk sway reduces the knee adduction moment by shifting the body’s center of mass closer to the stance limb. This decreases the lever arm of the ground reaction force relative to the knee, thereby unloading the medial compartment.
The same strategy also increases activation of the hip abductors, particularly the gluteus medius, to stabilize the pelvis and control frontal-plane motion. This strategy reduces hip adduction and the external hip adduction moment, thereby decreasing the mechanical demand on the hip joint and altering load distribution across periarticular structures.
Clinically, this can be taught by cueing runners to “bring your chest slightly over the stance leg.” Feedback can be delivered with mirrors, tactile prompts (such as a therapist’s hand on the trunk), or wearable sensors that vibrate when sway deviates from target values. The adjustment must remain modest, as exaggerated sway may cause compensatory issues or balance challenges.
4. Frontal-Plane Perturbation Gait Retraining
Introducing controlled side-to-side perturbations — such as treadmill shifts or uneven surfaces — forces the neuromuscular system to improve stability in the frontal plane. This training enhances hip abductor activation and trunk control, leading to more efficient load distribution.
Teaching involves progressive exposure, starting with small perturbations (e.g., balance boards or treadmill perturbations) and advancing to agility-based side shuffles or lateral hops. This trains stability under dynamic conditions relevant to real-world locomotion.
5. Lateral Wedge Insoles
Placing a wedge on the lateral side of the shoe promotes subtalar eversion and shifts the ground reaction force laterally during stance. This reduces the external knee adduction moment. Lateral wedge insoles have been shown to unload the medial knee compartment in osteoarthritis patients.
Teaching is straightforward: the insole is fitted into the runner’s shoe, and the clinician reassesses gait and comfort. Ongoing monitoring is needed, as some users may develop secondary discomfort in the ankle or hip.
6. Hip Abductor Strengthening
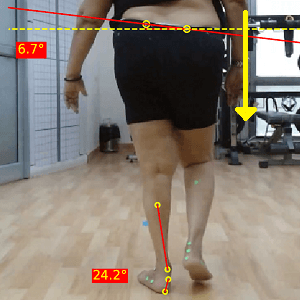
Fig: Increased pelvic drop
Weak hip abductors are strongly linked to excessive pelvic drop and hip adduction during stance, which increases medial knee and hip loads. Therefore, strengthening these muscles indirectly retrains gait by stabilizing the pelvis and reducing dynamic knee valgus.
Teaching involves progressing from isolated strengthening (e.g., side-lying leg raises, lateral band walks) to functional drills (e.g., resisted walking, single-leg squats) that replicate gait mechanics. Cues emphasize pelvic stability and alignment of the knee over the foot.
Additionally, visual feedback strategies like tying a colored band around the pelvis while walking in front of a mirror are also useful to minimize pelvic drop.
Transverse plane gait retraining strategies
1. Hip and Pelvic Rotation Control
Excessive femoral internal rotation and pelvic rotation are associated with patellofemoral joint stress and anterior knee pain. Retraining hip and pelvic control improves patellar tracking and reduces abnormal stress on the joint.
Teaching typically involves mirror or video feedback, with cues such as “keep your kneecap pointing straight ahead.” Or sticking tape/marker at the patella and cueing the same. Combining gait retraining with hip external rotator strengthening further supports lasting change. Combining this strategy with proprioceptive training can assist in achieving better outcomes.
2. Tibial Rotation and Foot Mechanics
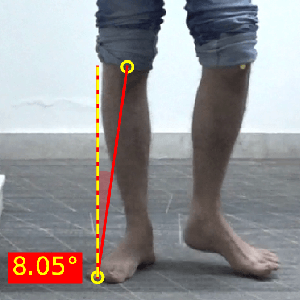
Fig: External tibial torsion
Small deviations in tibial rotation can meaningfully alter how forces are distributed across the knee joint, even without increasing ligament strain. When the tibia rotates internally, it increases medial and anterior knee loading, while external rotation tends to shift forces laterally and alter flexion torques. Over time, these subtle shifts in joint mechanics can contribute to uneven cartilage loading and potential degenerative changes.
Kinematically, it’s assessed by a line connecting the mid-point of the patella and the 2nd toe. A neutral patella and ab/adducted foot is an indicator of tibial torsion.
Retraining strategies include adjusting foot strike toward midfoot loading, strengthening intrinsic foot muscles, and improving ankle mobility. Teaching methods include barefoot walking drills on grass, video feedback of foot placement, and progressive strengthening exercises for the calf and foot.
3. Trunk–Pelvic Coordination
The relative motion of the trunk and pelvis in the transverse plane strongly influences how ground reaction forces are transmitted through the lower limb. Poor trunk–pelvis coordination can amplify knee adduction moments and rotational loading at the hip. Disrupted trunk–pelvis coordination shifts the body’s center of mass and alters load transfer, lengthening the ground reaction force lever arm at the knee and increasing torsional demands at the hip, thereby amplifying joint stress.
Trunk–hip separation, defined as the relative rotation between the trunk and pelvis, plays a central role in controlling transverse plane mechanics. Optimal separation allows efficient storage and release of elastic energy while maintaining balanced load distribution across the lower limb. However, excessive or poorly timed trunk–hip separation disrupts this balance, increasing shear and torsional stresses at the hip and altering knee loading patterns.
Retraining focuses on biofeedback and core stability drills. Clinicians may cue athletes to “move your shoulders and hips together” or “keep your trunk quiet while your legs move.” Exercises such as anti-rotation presses, banded trunk rotations, and rotational planks support better control.
4. Turning and Direction-Change Training
Running and walking rarely happen in straight lines. Additionally, gait is not a conscious activity, where individuals need to be aware of each step, surfaces, etc. It’s primarily intuitive, allowing other tasks to be performed alongside. Training pre-planned and reactive turns develops transverse-plane control and improves neuromuscular readiness for cutting or agility tasks.
Teaching often begins with cone drills, 45–90° turns, or agility ladder patterns, with cues to “turn your hips and shoulders together.” Over time, drills can progress to reactive cutting tasks, mimicking sport and real-world demands.
5. Core Rotational Stability Training
Training core stability directly improves trunk–pelvis coordination and reduces lower-limb loading.
Teaching includes exercises such as rotational medicine ball throws, anti-rotation holds, and cable trunk rotations. Cue athletes to maintain trunk alignment under load, progressing to dynamic drills like resisted running with torso stabilization.
Summary of Gait retraining strategies
|
Plane |
Strategy |
Biomechanical Rationale |
How to Teach / Apply |
|
Frontal |
Step Width Adjustments |
Wider steps reduce hip adduction and medial knee load |
Use tape lines, mirror/video feedback, cue “land slightly wider” |
|
Foot Progression Angle (Toe-in/out) |
Toe in -> Reduces medial knee loading |
Test angles with sensors/treadmill; cue “point toes slightly in/out” |
|
|
Trunk Lean & Sway |
Shifts COM over stance limb → reduces knee adduction moment |
Cue “chest over stance leg”; use mirror, tactile, or wearable feedback |
|
|
Perturbation Training |
Trains neuromuscular stability; strengthens hip abductors |
Begin with balance boards or treadmill perturbations, progress to lateral hops |
|
|
Lateral Wedge Insoles |
Shifts center of pressure laterally → reduces medial knee load |
Fit wedge insoles, reassess gait and comfort, monitor for compensations |
|
|
Hip Abductor Strengthening |
Stronger abductors stabilize pelvis → less knee valgus |
Side-lying raises, lateral band walks, progress to resisted walking drills |
|
|
Transverse |
Hip & Pelvic Rotation Control |
Reduces patellofemoral joint stress and maltracking |
Mirror/video feedback, cue “kneecap forward,” add hip rotator strengthening |
|
Tibial Rotation & Foot Mechanics |
Controls pronation and tibial over-rotation → lowers shin/foot strain |
Barefoot walking drills, video feedback, intrinsic foot strengthening |
|
|
Trunk–Pelvic Coordination |
Improves load transfer, lowers rotational stress at hip/knee |
Biofeedback; drills like Pallof press, rotational planks, banded trunk rotations |
|
|
Turning & Direction-Change Training |
Builds control in real-world scenarios where walking is not an isolated activity |
Cone drills, agility ladders, cue “turn hips/shoulders together,” progress to reactive cuts |
|
|
Core Rotational Stability Training |
Improves trunk control, reduces ACL and patellofemoral stress |
Rotational medicine ball throws, anti-rotation holds, resisted running with core control |
|
|
Neuromuscular Warm-Up Programs |
Multi-plane retraining reduces ACL injury risk |
Deliver as 15–20 min warm-up (e.g., FIFA 11+); include lunges, landings, cutting drills |
Practical tips for implementation of gait retraining
Assess all three planes – Don’t limit gait analysis to sagittal views. Even a simple frontal or overhead video can reveal step width, hip adduction, or pelvic rotation.
Use technology wisely – 3D gait labs are ideal, but wearable sensors, smart shoes, and even smartphone apps are making multi-plane analysis more accessible.
Personalize interventions – Not everyone benefits from the same cue. One person’s fix may worsen another’s load distribution.
Combine with strengthening – Especially for frontal and transverse retraining, hip abductors and core stabilizers play a huge role. Pair retraining with targeted strength programs.
Progress gradually – Gait changes are stressors. Introduce them slowly, monitor symptoms, and adjust load accordingly.
An accurate and objective assessment is very important. GaitON offers a comprehensive 2-D Gait analysis system to assess normal and pathological gait! To launch gait analysis at your center, contact us today!
ABOUT THE AUTHOR

GAYATRI SURESH (PT)
Gayatri Suresh (PT) is a Biomechanist who has completed her B.P.Th from DES College of Physiotherapy and M.P.T (Biomechanics) from SRM College of Physiotherapy, SRMIST. Her field of clinical expertise is in movement assessments through video analysis. Apart from her work at Auptimo, she works as a Clinical Specialist at Rehabilitation Research and Device Development, IIT Madras. She has won gold medals for her Research presentations and for securing First rank with distinction in her MPT degree respectively.
References
- Mündermann A, Asay JL, Mündermann L, Andriacchi TP. Implications of increased medio-lateral trunk sway for ambulatory mechanics. J Biomech. 2008;41:165–170.
- Uhlrich S, Mazzoli V, Kolesar J, et al. Personalised gait retraining for medial compartment knee osteoarthritis: a randomised controlled trial. Lancet Rheumatology. 2024.
- Andriacchi TP, et al. A framework for the in vivo pathomechanics of osteoarthritis at the knee. Ann Biomed Eng. 2004;32:447–457.
- Kerrigan DC, et al. Effectiveness of a lateral-wedge insole on knee varus torque in patients with knee osteoarthritis. Arch Phys Med Rehabil. 2002;83:889–893.
- Chang A, et al. Hip abduction moment and protection against medial tibiofemoral osteoarthritis progression. Arthritis Rheum. 2005;52:3515–3519.
- Zazulak BT, et al. Deficits in neuromuscular control of the trunk predict knee injury risk. Am J Sports Med. 2007;35(7):1123–1130.
- Yi Wan, Polly McGuigan, James Bilzon, Logan Wade. The effect of foot orientation modifications on knee joint biomechanics during daily activities in people with and without knee osteoarthritis. Clinical Biomechanics, Volume 117, 2024, 106287, ISSN 0268 0033, https://doi.org/10.1016/j.clinbiomech.2024.106287.
- Sample, Daniel & Thorsen, Tanner & Weinhandl, Joshua & Strohacker, Kelley & Zhang, Songning. (2020). Effects of Increased Step-Width on Knee Biomechanics During Inclined and Declined Walking. Journal of Applied Biomechanics. 36. 1-6. 10.1123/jab.2019-0298.
- Baghi R, Yin W, Badhyal S, Ramadan A, Oppizzi G, Li Z, Bowman P, Henn F, Zhang LQ. Determining the individual relationship between the step width and peak knee adduction moment during stepping in medial knee osteoarthritis. Clin Biomech (Bristol). 2025 Aug;128:106619. doi: 10.1016/j.clinbiomech.2025.106619. Epub 2025 Jul 22. PMID: 40737736; PMCID: PMC12368841.
- Bates NA, Nesbitt RJ, Shearn JT, Myer GD, Hewett TE. The influence of internal and external tibial rotation offsets on knee joint and ligament biomechanics during simulated athletic tasks. Clin Biomech (Bristol). 2018 Feb;52:109-116. doi: 10.1016/j.clinbiomech.2018.01.019. Epub 2018 Feb 2. PMID: 29425835; PMCID: PMC5835205.
- Mohammad WS, Elsais WM. Association Between Hip Rotation and Activation of the Quadriceps and Gluteus Maximus in Male Runners. Orthop J Sports Med. 2020 Nov 5;8(11):2325967120962802. doi: 10.1177/2325967120962802. PMID: 33225009; PMCID: PMC7653292.
The information found within this site is for general information only and should not be treated as a substitute for professional advice from a licensed medical practitioner. Any application of exercises and diagnostic tests suggested is at the reader’s sole discretion and risk.