Since footwear can hugely affect posture & biomechanics, a clinical shoe assessment of a patient is very important. An ‘incorrect’ pair of shoes can lead to several injuries, even if there is no physical limitation in the body.
The term ‘incorrect’, defines a shoe that is NOT suitable to the structure & function of the patient’s feet. Moreover, this term can also refer to shoes that can no longer assist the foot because of being damaged or worn out.
SHOE ASSESSMENT : REPLACEMENT GUIDELINES
[ To learn more about various biomechanical faults linked with running injuries along with their corrections, refer to this FREE running injuries course here. ]
Studies by (Asplund & Brown, 2005) (Furman, n.d.), have discussed guidelines on shoe replacement. Some of these are mentioned below:- After 300-500 miles of running or walking.
- Within 1 year of use, whether the shoe is worn out or not.
- Any signs of unevenness in the midsole, when placed on a flat surface.
- Any noticeable creasing in the Midsole.
- If the heel counter appears flexible when compressed from side to side
- If the heel counter appears deviated to one side when viewing from the rear of the shoe
- When the outer sole has worn through to midsole or there is more than 4mm difference between the medial & lateral side of the heel.
SHOE ASSESSMENT : PRESCRIPTION PROCESS
Since all feet are unique, there is a set of guidelines recommended by the American Academy of Podiatric Sports medicine (AAPSM) that can be helpful in shoe assessment & prescription.
As per Stephen M. Pribut, ex-president of AAPSM, a shoe prescription should be done keeping the following factors in mind. Although these factors are extremely relevant for running shoes, they should kept in mind while recommending walking shoes too.
- Biomechanical Needs
- Past experience with shoes
- Current Problems
- Environmental Factors
- Running & Racing Requirements
To address all these needs of the patient, a comprehensive examination of the foot & current footwear is necessary. In this blog, we will be discussing certain important factors that should be assessed in these examinations.
FOOT SIZE & SHOE FIT
Foot Length
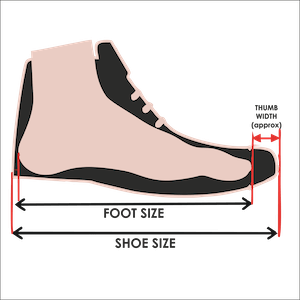
It’s important to ensure that the shoe is as per the length of the foot. Measurement of foot length should not only be limited to the overall length (heel to toe measurement), but also arch length (heel to first metatarsal head) measurement.
Shoes are designed to flex at the ‘ball’ of the foot. Therefore, the first metatarsal joint should be positioned in the widest part of the shoe. This provides room for the toes so they are not confined. Besides, an adequate lacing system or adjustable strap is also helpful in obtaining a required fit. (McWhorter, et al., 2003)
As a general rule, having a thumb’s width in space beyond the end of the longest toe to the tip of the shoe ensures a good fit. (Langone, 2010)
Foot Width
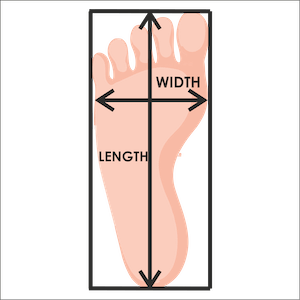
In addition to foot length, foot width is another factor that is often neglected during shoe assessment. Both foot length & foot width can be easily measured using a Brannock® device. (Buldt & Menz, 2018)
Although awareness is increasing, many patients are still unaware of the need for wider shoes to address foot deformities like bunions or hammertoes.
However, a positive trend in athletic shoes over recent years has been the availability of various width options. Brands like New Balance, Asics, Orthofeet offer a full range of narrow, medium & wide widths to help patients with foot width related issues.
- Adequate depth over joints & toes is important to allow free movement. This is particularly important at toe taper to eliminate pressure over the dorsal deformity aspect of the toes and nails
- Feet are not perfect matches. One foot is always a little bigger than the other. In such cases, it’s always good to fit the shoe to the larger foot.
- As studied by (McWhorter, et al., 2003), the volume of the foot increases by 3% after 10 minutes of light running on a treadmill. Hence, it is important to take measurements after exercise.
HEEL COUNTER

TORSION CONTROL

FOREFOOT FLEXIBILITY & MIDFOOT STABILITY
This parameter is probably the most important factor in athletic shoe assessment. Like heel counter stiffness and torsion control, it is also a part of the three-point testing methodology by AAPSM.
The test evaluates the ease of flexion of the most distal third of the shoe as well as the flexion resistance of the middle third of the shoe. (Williams, 2010)
Forefoot flexibility

Midfoot Stability

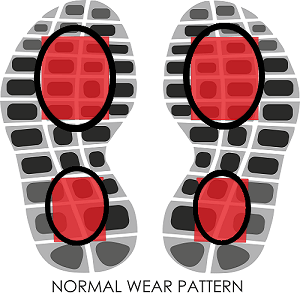
ASSESSMENT OF SHOE WEAR PATTERN
Pressure under the sole of the shoe should generally be even, with no excessive wear in any particular region. Additionally, normal wear should occur at the lateral heel (where your foot first hits when you walk) and medial central forefoot (where you push off when you step).
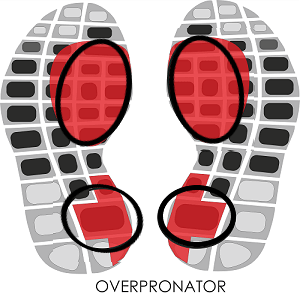
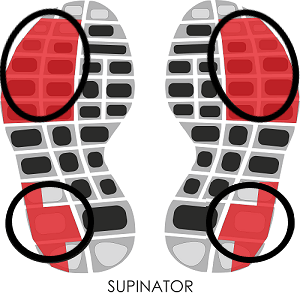
ADDITIONAL WEAR PATTERNS (Williams, 2007)
- The absence of wear at the tip of the sole of an old and worn shoe may indicate a lack of push-off during the gait cycle.
- Excessive forefoot wear indicates ankle joint equinus
- Circular forefoot wear over the first metatarsophalangeal joint is present in pes cavus deformity.
MIDSOLE DENSITY VARIATIONS
ASSESSMENT OF SHOE LAST
The last describes the shape of the shoe. Generally, there are three kinds of lasts.
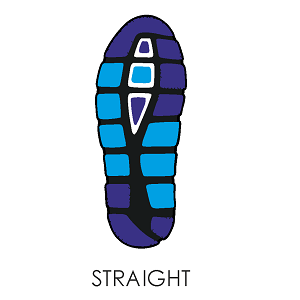
Straight-last: More resistant to pronation, heavier, & often incorporate a controlling medial post.
These are found almost exclusively in motion-control shoes.
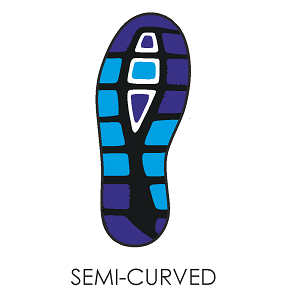
Semi curved last: Intermediate between straight lasted and curve-lasted.
These are found in most running shoes
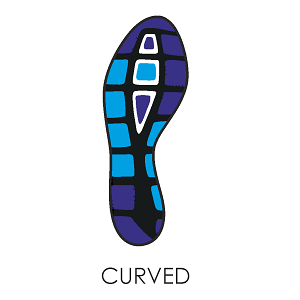
Curve-last: Lighter, more cushioned, & offer minimal resistance to pronation.
These are commonly found in competition shoes, cushioned, and neutral shoes
TYPES OF RUNNING SHOES (Langone, 2010)
Neutral shoes: These shoes provide a blend of cushioning, medial support, and durability. Semi curved last (to offer hindfoot stability and forefoot flexibility). They often have a medial post or multi-density midsole to provide a degree of pronation control. Well suited to the midweight runners & people with neutral pronation and medium-to-low arches.
Motion Control Shoes: These shoes provide the maximum pronation resistance, stiff heel counter, high torsion resistance, stiff medial midsole, rigid medial post & Straight last. Benefit heavyweight runners or runners with a low arch or an overpronated foot.
Cushioned shoes High Arch / Supinated foot: These shoes provide the minimal pronation resistance, higher flexibility, soft & cushioned midsole, least medial support & curved last. Benefit light to midweight runners & runners with High Arch / Supinated foot.
SOME SPECIFIC PROBLEMS THAT INFLUENCE SHOE ASSESSMENT
As we discussed above, previous injury history can hugely affect the process of shoe assessment & prescription.
For eg, patients with previous stress fractures benefit from greater cushioning in the shoes. On the other hand, a runner with a history of Achilles tendinopathy may require a shoe with firm midsoles and ample heel elevation. (Richie Jr., 2008)
It is important to keep following up with patients and take their feedback. A lot of clinicians use video gait analysis to quantify the changes in the walking or running pattern due to the footwear.
Needless to say, a detailed injury history & physical examination of the patient are extremely helpful in effective shoe recommendation.
In conclusion, a new shoe is a big biomechanical change introduced in the body. Hence, shoe assessment and prescription should be an informed decision done by considering all factors into account.
Since you’re here…
…we have a small favor to ask. More people are reading our blogs everyday, and each week we bring you compelling content to help you treat your patients better. Please take a moment to share the articles on social media, engage the authors with questions and comments below, and link to articles when appropriate if you have a blog or participate on forums of related topics. — Team Auptimo
ABOUT THE AUTHOR
SIDDHARTH HANS
With over 4 years of experience in biomechanical analysis, Siddharth is the product manager of GaitON. He has been certified in the courses of ‘Running Mechanics for clinicians’, ‘Common biomechanical errors seen in runners’, ‘Rehabilitation of running biomechanics’.
REFERENCES:
A-M
- Asplund, . C. A. & Brown , D. L., 2005. The Running Shoe Prescription. The Physician and Sportsmedicine, 33(1), pp. 17-24.
- Buldt, A. K. & Menz, H. B., 2018. Incorrectly fitted footwear, foot pain and foot disorders: a systematic search and narrative review of the literature. J Foot Ankle Res..
- Furman, A., n.d. How Do I Know When It Is Time To Replace My Athletic Shoes?. [Online]
Available at: http://www.aapsm.org/replace_shoes.html
[Accessed 30 April 2020]. - Langone, K. . A., 2010. How to Evaluate and Recommend Athletic Shoes. PODIATRY MANAGEMENT, October.
- Levine, D., 2010. Athletic Shoe Evaluation. In: M. B. Werd & E. L. Knight, eds. Athletic Footwear and Orthoses. s.l.:s.n.
- McWhorter , J. W. et al., 2003. The effects of walking, running, and shoe size on foot volumetrics. Physical Therapy in Sport.
N-Z
- Richie Jr., D., 2008. Recommending Athletic Footwear For Runners. [Online]
Available at: https://www.podiatrytoday.com/article/8789
[Accessed 28 April 2020]. - Stacoff, A., Reinschmidt, C. & Stüssi, E., 1992;. The movement of the heel within a running shoe.. Med Sci Sports Exerc, 24(6), pp. 695-701.
- Werd, M. B. & Knight, E. L., 2010. Prescribing Athletic Footwear and Orthoses: The Game Plan. In: M. B. Werd & E. L. Knight, eds. Athletic Footwear and Orthoses. s.l.:s.n.
- Williams, A., 2007. Footwear Assessment and Management. Podiatry Management, October.
- Williams, B. E., 2010. A three-point approach to testing running shoes. [Online]
Available at: https://lermagazine.com/article/a-three-point-approach-to-testing-running-shoes
[Accessed 29 April 2020].
Nice article and informative one.
Thank you for your appreciation! We are glad you found it useful